













 337 / 509
337 / 509

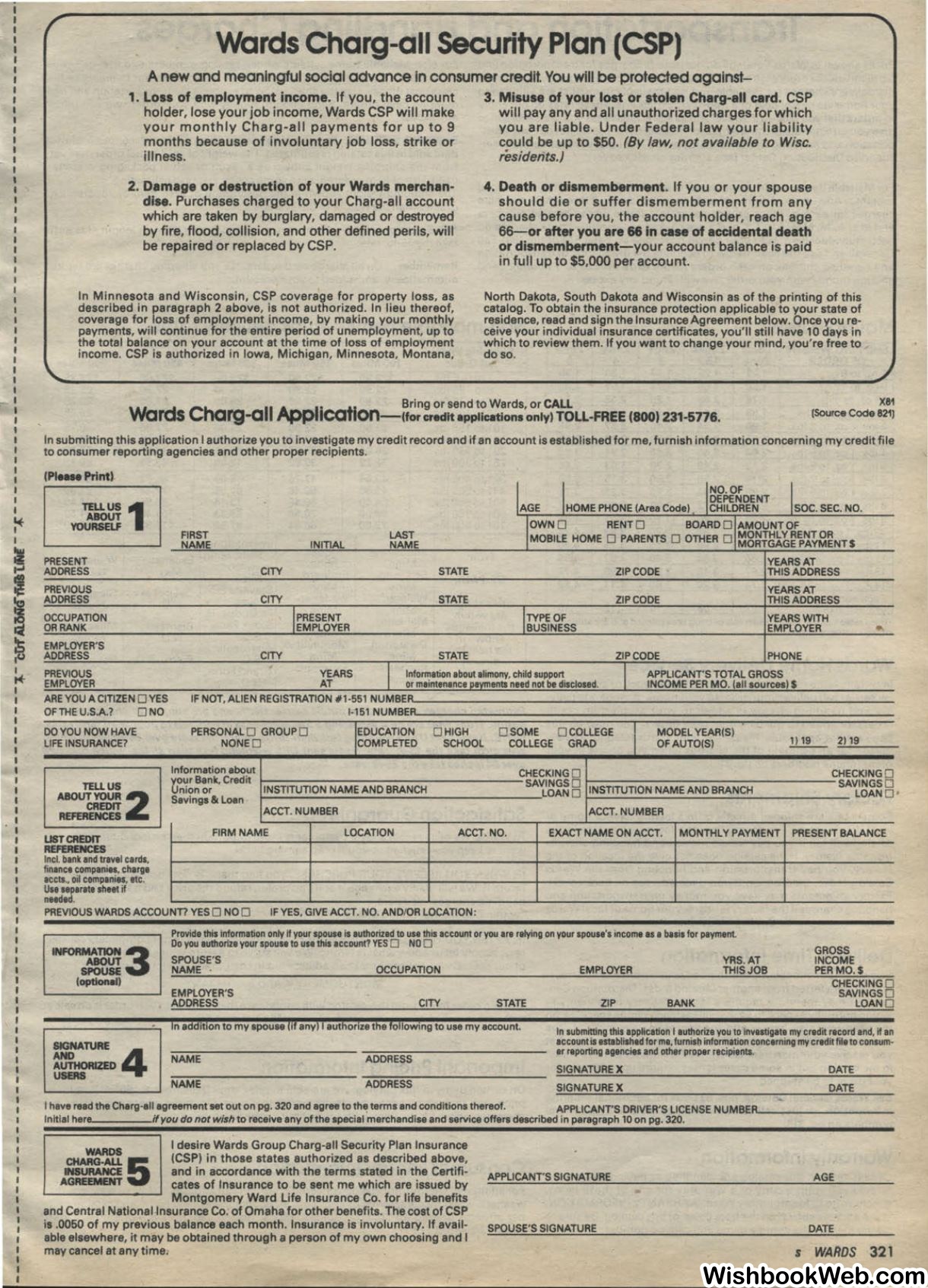
Wards Charg-all Security Plan (CSP)
Anew and meaningful social advance In consumer credit. You will
be
protected against-
1.
Loss of employment income. If you, the account
holder, lose your job income, Wards CSP will make
your monthly Charg-all payments for up to
9
months because of involuntary job loss, strike or
illness.
2.
Damage or destruction of your Wards merchan–
dise. Purchases charged to your Charg-all account
which are taken by burglary, damaged or destroyed
by fire, flood, collision, and other defined perils, will
be repaired or replaced by CSP.
In Minnesota and Wisconsin, CSP coverage for property loss, as
described in paragraph 2 above, is not authorized. In lieu thereof,
coverage for loss of employment income, by making your monthly
payments, will continue for the entire period of unemployment, up to
the total balance on your account at the time of loss of employment
income. CSP is authorized in Iowa, Michigan, Minnesota, Montana,
3. Misuse of your lost or stolen Charg-all card. CSP
will pay any and all unauthorized charges for which
you are liable. Under Federal law your liability
could be up to
$50.
(By
law, not available to Wisc.
residents.)
4.
Death or dismemberment. If you or your spouse
should die or suffer dismemberment from any
cause before you, the account holder, reach age
66-or after you are 66 in case of accidental death
or dismemberment-your account balance is paid
in full up to
$5,000
per account.
North Dakota, South Dakota and Wisconsin as of the printing of this
catalog. To obtain the insurance protection applicable to your state of
residence, read and sign the Insurance Agreement below. Once you re–
ceive your individual insurance certificates, you'll still have
10
days in
which to review them. If you want to change your mind, you're free to
do so.
Bring or send to Wards, or
CALL
Words Charg-all
Appllcatlon-1tor credit
applications only)
TOLL-FREE
(800) 231-5776.
X81
(source
Code 821)
In submitting this application I authorize you to investigate my credit record and if an account is established for me, furnish information concerning my credit file
to consumer reporting agencies and other proper recipients.
IAGE
IHOME PHONE (Area Code)
INO.OFI
soc.
SEC. NO.
DEPENDENT
TELLUS
1
CHILOREN
ABOUT
IOWN O
RENT O
BOARD ~tMOUNTOF
YOURSELF
FIRST
LAST
MONTHLY RENT OR
NAME
INITIAL
NAME
MOBILE HOME 0 PARENTS 0 OTHER 0 MORTGAGE PAYMENTS
PRESENT
YEARS AT
ADDRESS
CITY
STATE
ZIP CODE
THIS ADDRESS
PREVIOUS
YEARS AT
ADDRESS
CITY
STATE
ZIP CODE
THIS ADDRESS
OCCUPATION
I
PRESENT
ITYPEOF
YEARS WITH
OR RANK
EMPLOYER
BUSINESS
EMPLOYER
•
EMPLOYER'S
ADDRESS
CITY
STATE
ZIP CODE
PHONE
PREVIOUS
YEARS
I
Information about alimony, child support
I
APPLICANT'S TOTAL GROSS
EMPLOYER
AT
or maintenance payments need not be disclosed.
INCOME PER MO. (all sources)$
ARE YOU A CITIZEN
0
YES
IF NOT, ALIEN REGISTRATION
#1·551
NUMBE:"--------------------------------
OF THE U.S.A.?
O NO
1-151
NUMBE"
DO
YOU NOW HAVE
PERSONAL O GROUP O
'EDUCATION
O HIGH
O SOME
O COLLEGE
I
MODEL YEAR(S)
2119
LIFE INSURANCE?
NONE O
COMPLETED
SCHOOL
COLLEGE GRAD
OFAUTO(S)
.!l.!L
Information about
CHECKING O
CHECKING O
TELL
US
r,ol!r Bank. Credit
INSTITUTION NAME AND BRANCH
SAVINGS O
INSTITUTION NAME AND BRANCH
SAVINGS O
n1on or
LOAN O
LOAN O
ABOUTYOUR2
Savings
&
Loan
CREDIT
ACCT. NUMBER
ACCT. NUMBER
REFERENCES
USTCREDIT
FIRM NAME
LOCATION
ACCT. NO.
EXACT NAME ON ACCT.
MONTHLY PAYMENT PRESENT BALANCE
REFERENCES
Incl. bank and travel cerds.
fin1nc1 companies, charge
1ccts.. oil companies, etc.
~::::!.""'
111111
~
PREVIOUS WARDS ACCOUNTI YES
0
NO
0
IF YES, GIVE ACCT. NO. AND/OR LOCATION:
INFORMA..=3
SPOUSE
(optional)
Provide this information only
n
your spouse is authorized
ta
uso this account or you
ore
relying on your spouse's income
IS
a
b11is for payment.
Do you 1uthoriz1 your spouse to use this account? YES 0 NO 0
SPOUSE'S
YRS. AT
NAME •
OCCUPATION
EMPLOYER
THISJOB
EMPLOYER'S
ADDRESS
CITY
STATE
ZIP
BANK
GROSS
INCOME
PERMO. S
CHECKING O
SAVINGS O
LOAN O
~NATURE
4
AUTHORIZED
USERS
In addition to my spouae (if any) I authorize the foUowing to use my account.
NAME
ADDRESS
In submitting this application I authorize you to investigate my credit record and, nan
account is established for me. furnish information concerning my credit file to consum–
er reporting agencies and other proper recipients.
SIGNATUREX
DATE
NAME
ADDRESS
SIGNATUREX
DATE
Ihave read the Charg-alf agreement
set
out on pg.
320
and agree to the terms and conditions thereof.
APPLICANT'S DRIVER'S LICENSENUMBE"---------
lnltial her
if
you do not wish
to receive any of the special merchandise and service offers described in paragraph
10
on pg.
320.
WARDS
CHARG·ALL
5
INSURANCE
AGREEMENT
I desire Wards Group Charg-all Security Plan Insurance
(CSP) in those states authorized as described above,
and in accordance with the terms stated in the Certifi–
cates of Insurance to be sent me which are issued by
Montgomery Ward Life Insurance Co. for life benefits
and Central National Insurance Co. of Omaha for other benefits. The cost of CSP
is .0050 of my previous balance each month. Insurance is involuntary. If avail–
able elsewhere, it may be obtained through a person of my own choosing and I
may cancel at any time.
APPLICANT'S SIGNATURE
SPOUSE'S SIGNATURE
AGE
DATE
s
WARDS
321