













 371 / 489
371 / 489

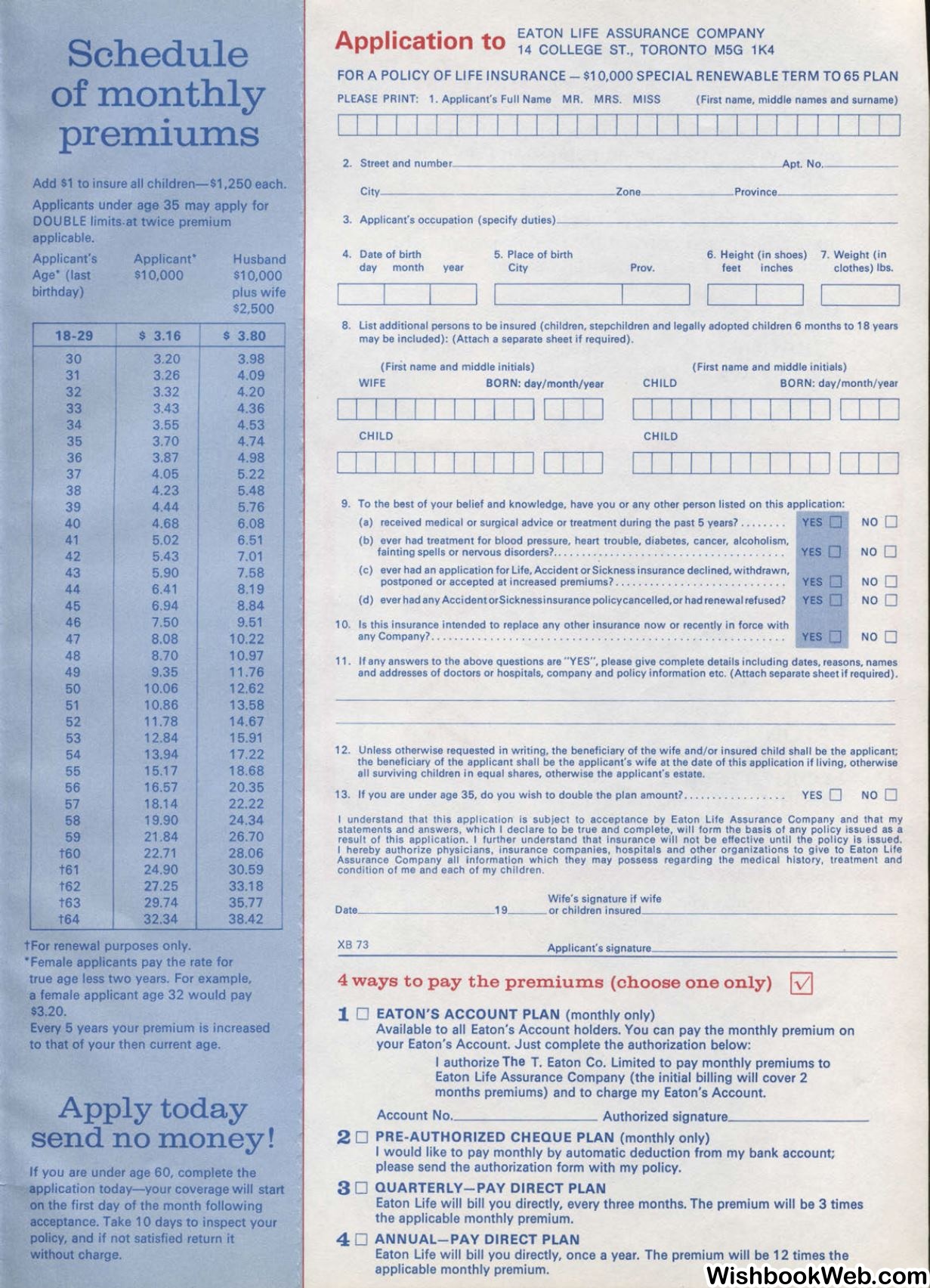
Schedule
of monthly
•
preinIUlllS
Add $1 to insure all children-$1,250 each.
Applicants under age 35 may apply for
DOUBLE
limits.attwice premium
applicable.
Applicant's
Age' (last
birthday)
18-29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
t60
t61
t62
t63
t64
Applicant*
$10,000
$
3.16
3.20
3.26
3.32
3.43
3.55
3.70
3.87
4.05
4.23
4.44
4.68
5.02
5.43
5.90
6.41
6.94
7.50
8.08
8.70
9.35
10.06
10.86
11.78
12.84
13.94
15.17
16.57
18.14
19.90
21.84
22.71
24.90
27.25
29.74
32.34
tFor renewal purposes only.
Husband
$10,000
plus wife
$2,500
$
3.80
3.98
4.09
4.20
4.36
4.53
4.74
4.98
5.22
5.48
5.76
6.08
6.51
7.01
7.58
8.19
8.84
9.51
10.22
10.97
11 .76
12.62
13.58
14.67
15.91
17.22
18.68
20.35
22.22
24.34
26.70
28.06
30.59
33.18
35.77
38.42
*Female applicants pay the rate for
true age less two years. For example,
a female applicant age 32 would pay
$3.20.
Every 5 years your premium is increased
to that of your then current age.
Apply today
send no money!
If you are under age 60, complete the
application today-your coverage will start
on the first day of the month following
acceptance. Take 10 days to inspect your
policy, and if not satisfied return it
without charge.
Application to
EATON LIFE AssuRANcE coMPANY
14 COLLEGE ST., TORONTO MSG 1K4
FOR A POLICY OF LIFE INSURANCE - $10,000 SPECIAL RENEWABLE TERM TO 65 PLAN
PLEASE PRINT: 1. Appl icant's Full Name MR. MRS. MISS
(First name, middle names and surname)
I I
I
I
2. Street and number______________________Apt. No,_____
City________ ______ __zone______Province________
3. Applicant's occupation (specify duties)---------- -------------
4. Date of birth
5. Place of birth
City
6. Height (in shoes) 7. Weight (in
day month
year
Prov.
feet
inches
clothes) lbs.
..___._____.I
~I
-~
8. List additional persons to be insured (children, stepchildren and legally adopted children 6 months to 18 years
may be included): (Attach a separate sheet if required).
(First name and middle initials)
(First name and middle initials)
WIFE
BORN: day/month/year
CHILD
BORN: day/month/ year
I I
I
I
I
I
I I I I
I
I I I
I
I I
CHILD
CHILD
I
I
I I
I
I
I I I
I I
I I
I
I I
9. To the best of your belief and knowledge, have you or any other person listed on this application:
(a) received medical or surgical advice or treatment during the past 5 years?... . . . . . YES D
NO D
(b) ever had treatment for blood pressure, heart trouble, diabetes, cancer, alcoholism,
fainting spells or nervous disorders?.... . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
YES
0
(c) ever had an application for Life, Accident or Sickness insurance declined, withdrawn,
postponed or accepted at increased premiums? ... . . . .... . ........ . . .. . .... YES D
(d) ever had any AccidentorSicknessinsurance policycancelled,or had renewal refused?
YES D
NO D
NO D
NO D
10. Is this insurance intended to replace any other insurance now or recently in force with
any Company? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
YES D
NO D
11 . If any answers to the above questions are " YES", please give complete details including dates, reasons, names
and addresses of doctors or hospitals, company and policy information etc. (Attach separate sheet if required) .
12. Unless otherwise requested in writing, the beneficiary of the wife and/ or insured child shall be the applicant;
the beneficiary of the applicant shall be the applicant's wife at the date of this application if living, otherwise
all surviving children in equal shares, otherwise the applicant's estate.
13. If you are under age 35, do you w ish to double the plan amount? .. .. .. . .. ... . .. . .
YES D
NO D
I understand that this appli cation is subject to acceptance by Eaton Life Assurance Company and that my
statements and answers, whi ch I declare to be true and complete, will form the basis of any policy issued as a
result of this application. I further understand that insurance will not be effective until the policy is issued.
I hereby authorize physicians, insurance companies, hospitals and other organizations to give to Eaton Life
Assurance Company all information which they may possess regarding the medical history, treatment and
condition of me and each of my children.
Wife's signature if wife
Date,___ ______19___ or children insured,_________________
XB 73
Applicant's signature
4 ways to pay the premiums (choose one only)
52]
1
0
EATON'S ACCOUNT PLAN (monthly only)
Available to all Eaton's Account holders. You can pay the monthly premium on
your Eaton's Account. Just complete the authorization below:
I authorize The T. Eaton Co. Limited to pay monthly premiums to
Eaton Life Assurance Company {the initial billing will cover 2
months premiums) and to charge my Eaton's Account.
Account No.
Authorized signature_________
2
0
PRE-AUTHORIZED CHEQUE PLAN (monthly only)
I would like to pay monthly by automatic deduction from my bank account;
please send the authorization form with my policy.
3
0
QUARTERLY-PAY DIRECT PLAN
Eaton Life will bill you directly, every three months. The premium will be 3 times
the applicable monthly premium.
4 0
ANNUAL-PAY DIRECT PLAN
Eaton Life will bill you directly, once a year. The premium will be 12 times the
applicable monthly premium.